Category: Uncategorized
Beyond the Bedside: Why Leadership Development is Your Highest ROI Retention Strategy
By Derek Bell, MS, CWP, Vice President of Solutions & Clinical Operations at VITAL WorkLife
In the current healthcare landscape, “staffing” has been reframed. It is no longer a simple HR headcount metric; it is a defensible patient safety obligation. As new Joint Commission standards take effect, the pressure on healthcare organizations to maintain a stable, engaged workforce has reached a fever pitch.
But here is the hard truth: You cannot “recruit” your way out of a retention crisis.
The most significant lever for workforce stability isn’t found in a sign-on bonus—it’s found in the quality of your leadership. In healthcare, leaders are the “Human Front Door” of the organization. When they flourish, their teams follow. When they struggle, the resulting “turnover tax” can devastate a hospital’s financial resilience.
The Shift from Burnout to Flourishing
For years, the industry has focused on “burnout prevention”—a reactive, deficit-based model that attempts to stop the bleeding. To achieve long-term ROI, we must move toward a proactive culture of flourishing. Flourishing isn’t a vague “wellness” concept; it is an evidence-based framework consisting of six critical and interdependent domains:
- Mental & Physical Health
- Meaning & Purpose
- Character & Virtue
- Close Social Relationships
- Financial & Material Stability
- Happiness & Life Satisfaction
Leadership development is the bridge that carries an organization across these domains. When we invest in developing leaders, we are investing in the very infrastructure that supports these six pillars for the entire workforce.
The ROI of the “Human Factor”
Why is leadership development the best return on investment for retention?
- Reducing the Turnover Tax. The cost of replacing a single physician or specialized nurse can range from $250,000 to more than $1 million when factoring in recruitment, onboarding, and lost clinical revenue. Leadership development acts as a preventative measure. Leaders equipped with high emotional intelligence and “human factor” training create psychological safety, which is the top predictor of team retention.
- Moving from Intuition to Insights. Modern leadership development replaces “gut-feeling” management with data-driven insights. By understanding organizational maturity stages, leaders can identify risk signals in their teams before those signals turn into resignations.
- Cultivating the “Digital Front Door.” In a decentralized healthcare world, leaders must be the champions of frictionless support. Whether it is specialty-matched peer coaching or 24/7 mental health access, leaders who are trained to promote these resources ensure that their teams feel supported at the point of need.
Co-Designing a Sustainable Future
The new normal of healthcare delivery requires a new kind of leader—one who understands that professional development and personal well-being are inextricably linked.
By prioritizing leadership development, organizations are doing more than just filling gaps in a schedule. They are co-designing a future where clinicians don’t just survive the shift—they flourish in their careers.
As we look ahead in 2026, the question for C-suite leaders is no longer “Can we afford to develop our leaders?” The question is “Can we afford the cost of a leader who isn’t prepared to lead?”
VITAL WorkLife empowers the human side of healthcare by supporting the entire workforce—from the bedside to the boardroom—at the intersection of people, performance, and well-being. To learn more about the flourishing framework, visit VITALWorkLife.com.
Learning in the Flow of Work: Continuous Development
By LAK Group
For many years, organizational learning was treated as an event: classrooms, workshops, multi-hour webinars, and long e-learning modules. People left their day-to-day responsibilities, attended a program, and then tried, often with mixed success, to apply what they had learned back on the job. Valuable? Yes. But in today’s faster, more complex environment, this model on its own is no longer enough.
That’s where the idea of learning in the flow of work comes in. Popularized by Josh Bersin, the concept is simple but powerful: instead of pulling employees away from their work to learn, we design learning so it happens while they are working, at the moment of need, in the context of real tasks, and in ways that are quick, relevant, and easy to access.
What Do We Mean by “Learning in the Flow of Work”?
Learning in the flow of work is about giving people “just enough” learning, “just in time,” so they can use it immediately. Rather than a separate activity reserved for training days, development becomes a natural part of everyday execution.
In practice, this can look like a manager pulling up a short conversation guide before delivering difficult feedback, a leader using an AI-enabled tool to rehearse a tough conversation, or a team accessing a quick decision framework while working through a complex problem. The common thread is that learning is embedded in real work, not abstracted away from it.
This approach matters because modern work rarely slows down. Organizations are navigating constant change, new technologies, shifting customer expectations, and evolving employee needs. Teams have limited capacity to step out for lengthy programs, but they still need to grow. Learning in the flow of work helps close the gap between “I know this” and “I actually used this,” which is where most traditional training falls short.
Why Learning in the Flow of Work Matters Now
Three realities make this approach especially important today. First, work is fast-moving. Business priorities shift quickly, and leaders often feel they cannot afford to take people out of the operation for large chunks of time. Second, work is increasingly complex and distributed. Hybrid and remote teams, new tools, and cross-functional collaboration all create scenarios in which the “right way” to act is highly contextual and constantly evolving. Finally, organizations are under pressure to show real impact from learning and development investments. It’s no longer enough to track attendance; stakeholders want to see behavior change and business results.
By embedding learning into everyday workflows, organizations increase the likelihood that new ideas are applied immediately, reinforced over time, and connected directly to performance. Research has long shown that people retain more when they can practice and apply new skills in context, not just hear about them in theory.
What Learning in the Flow of Work Looks Like
A common misconception is that learning in the flow of work requires a wholesale redesign of all programs. In reality, it often starts with small, practical shifts.
Some organizations begin by creating job-embedded tools: short guides, checklists, or templates that sit as close as possible to the work itself. For example, a one-page framework for giving feedback, a set of coaching questions for one-on-one meetings, or a quick reference for handling difficult customer situations. When these resources are easy to find and simple to use, employees are far more likely to apply them.
Others focus on integrating real-time coaching and feedback into existing rhythms. Instead of waiting for annual programs, leaders and coaches work with people on live challenges: preparing for a specific conversation, debriefing a key meeting, or reflecting on a recent decision. This turns real work into the primary learning lab.
Short, focused “micro-learning” experiences also play a role. These might be five- to ten-minute modules or brief videos that are timed to upcoming tasks, “before your next 1:1,” “before your next client presentation,” or “before you run that performance discussion.” The key is that content is targeted, practical, and immediately usable.
Increasingly, technology is a critical enabler. Learning platforms can integrate with calendars, collaboration tools, and performance systems to surface relevant resources at the right time. Generative AI can help leaders draft feedback, rehearse conversations, and explore “what if” scenarios in a safe environment, providing low-risk practice opportunities that complement human coaching rather than replacing it.
The Crucial Role of Leaders
No matter how good the tools or content are, learning in the flow of work succeeds or fails based on leadership behavior.
When leaders treat learning as a separate, optional activity, employees will do the same. But when leaders consistently pause to ask questions like “What did we learn from this?” or “How will we handle this differently next time?” they send a powerful signal that reflection is part of the job, not a luxury.
Leaders who share their own learning openly, admitting mistakes, naming insights, and modeling new behaviors, make it safer for others to do the same. Over time, this builds a culture in which learning is not an event but an ongoing practice woven into meetings, decisions, and day-to-day interactions.
Getting Started: A Practical Approach
The good news is that you do not need a massive change program to begin moving toward learning in the flow of work. A practical way to start is to choose one critical moment in your organization’s work and focus there. It might be onboarding, performance conversations, sales meetings, or project kick-offs, any situation where better preparation and reflection would clearly improve outcomes.
From there, ask where people feel stuck or unprepared and design one or two simple supports: a guide, a short learning resource, a targeted coaching touchpoint, or an AI-enabled tool that offers structure and language in the moment of need. Pilot with a small population, gather feedback on whether the support helped “in the moment,” and refine from there. Over time, you can add more moments and more layers, gradually building a learning ecosystem that is truly integrated into work.
Call to Action: Partner with LAK Group
At LAK Group, we help organizations move from event-based learning to integrated, real-time development by combining leadership coaching, talent assessment, and modern learning design. Our work is grounded in helping leaders and teams learn while they work, through coaching in the flow of real challenges, AI-enabled practice experiences, and programs that are tightly connected to your strategy.
If you’re ready to explore how learning in the flow of work could look in your organization, starting with a focused pilot or a leadership cohort, we’d be glad to talk.
Let’s design a learning experience that meets your people where they work. Contact LAK Group to schedule a conversation about learning in the flow of work and what it could mean for your leaders, teams, and business.
References
- Bersin, J. (2018). A New Paradigm For Corporate Training: Learning In The Flow Of Work.
- Center for Creative Leadership. (n.d.). The 70-20-10 Rule for Leadership Development – emphasizing the importance of on-the-job experiences in driving growth.
- Deloitte Human Capital Trends. (Various years). Findings consistently highlight the need for continuous, integrated learning in response to rapid organizational change.
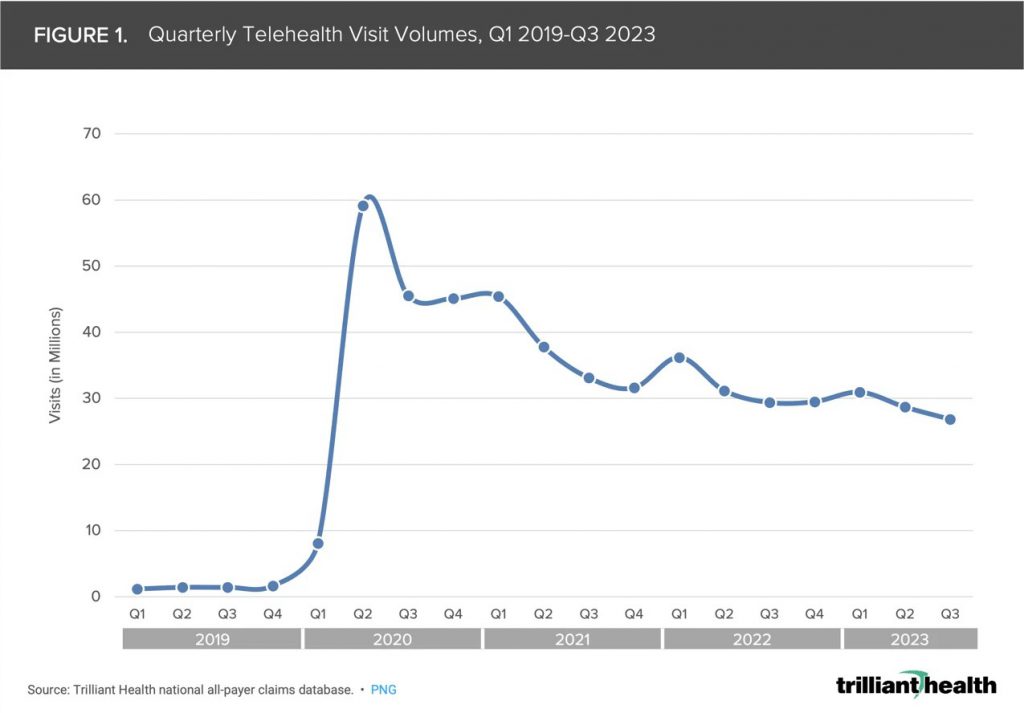
Telemedicine and Its Impact on Healthcare Planning

Introduction
While access to virtual healthcare platforms has been on the rise in recent years, the impact of COVID-19 has accelerated that trend, encouraged by restrictions on office visits and in some instances, reduced or zero insurance copays required by healthcare systems. Patients are realizing more convenient access to healthcare, while avoiding the need to interact with other sick patients, leading to higher satisfaction and loyalty. Providers can better manage privacy concerns and missed appointments, while still scheduling in person visits where most appropriate, thus leading to greater efficiency and satisfaction. The healthcare network is able to expand access into the community, and work toward improved quality measures and outcomes. However, Medicare restrictions and private insurance coverage has not always caught up to these changes, and are still adjusting their administrative policies.
As defined by the American Academy of Family Physicians, “telemedicine” is clinical services delivered by a physician at a remote location, while “telehealth” includes broader scope of remote non-clinical services such as training and patient education. Telemedicine includes delivering care to patient within their current system via real-time communication, but could also utilize remote clinical services of a specialist brought onto the care team, which may occur at small, rural hospitals. This article will primarily focus on virtual care within a pre-existing patient / provider relationship.
A recent report from McKinsey and Company projects a rise in telehealth services could eventually result in a shift of $250 billion of current US healthcare costs. This could eventually include 20% of ED visits and 24% of outpatient office visits. Increased utilization of wearable devices to monitor pre-existing health conditions may also contribute to these trends.
According to the AMA Telehealth Implementation Playbook and the American Academy of Family Physicians, telemedicine is most appropriate for simple and low-risk diagnoses requiring a prescription (i.e. colds and flu, UTI’s), follow up and recurring care to manage chronic conditions, behavioral health counseling and medication management, other routine appointments, and for people with transportation difficulties. If these projections are realized, healthcare planning will certainly need to consider and accommodate these impacts.
Planning Considerations
The 2018 edition of Guidelines for Design and Construction of Outpatient Facilities greatly expanded on the recommendations for design of spaces devoted to telemedicine services. However, they state in the Appendix that, “The requirements in this section are not intended to apply to virtual visits that do not require a physical examination of the patient or visits that originate from a physician’s or patient’s home.” Regardless, their recommendations are useful for all types of virtual care, as they speak to the environmental characteristics suggested for effective delivery of care in a remote setting.
Telemedicine can also take two paths: consultation with the patient’s primary care provider, or by a physician or other healthcare professional dedicated to virtual appointments. In either instance, care is not being delivered in a physical office, and therefore, program needs are impacted. These are some areas to consider when a portion of the patient volume is diverted:
- Are fewer parking spaces needed?
- Waiting room size: does a smaller in-person caseload reduce delays in the waiting room, or will social distancing concerns just spread-out waiting patients?
- Exam rooms – review and respond to daily patient volumes and trends, rather than basing need on number of providers or past experience.
- How are changes in workflow accommodated, such as access to electronic medical records by a physician other than the patient’s care provider? Are fewer nursing and support staff needed?
- How will virtual visits impact secondary diversions from Urgent Care and ED?
Program Needs

It is critical that spaces designed to provide telemedicine services does not distract or compromise the provider’s ability to provide the same high-quality level of care as an in-person encounter. Not only does the provider need to project a professional image in their appearance and body language, but the environment where a virtual encounter takes place needs to be carefully considered. First, will the space be located where provider can easily access without disrupting the daily flow of activities, and still maintain a sufficient level of privacy and focus? If such a space is being retrofit in an existing clinic, a consultation space may be more suitable than an exam room or doctor’s private office.
The technology for virtual meeting platforms is evolving quickly, and so infrastructure must be designed for flexibility. Patients may be using an app on their phone or other portable device, and bandwidth limitations should be considered so that calls are not lost in the middle of the visit. Patient confidentiality also means concerns regarding cybersecurity must be addressed.
Once space is identified, appropriate lighting and acoustics need to enable patient to communicate without distractions or concerns over confidentiality. The background should be a neutral, non-glossy color with minimal visual clutter. Camera should be positioned at eye level to encourage personal interaction.
Conclusion
Although the arrival of telemedicine has been anticipated for several years now, the impact of COVID-19 may encourage patients to embrace virtual care permanently. While still evolving, it can never fully replace the traditional care model. The ability to address minor or ongoing care issues remotely will allow providers to focus their efforts, and identify early on when more personal intervention is needed.
 About the Author: Michael Schaefer, AIA, NCARB, CCCA, LEED AP
About the Author: Michael Schaefer, AIA, NCARB, CCCA, LEED AP
Michael has been with PRA since 1994, and since then worked in various studios but specializes in
Healthcare. Michael’s passion for creating healthy living environments is incomparable to anyone
else. He feels a large responsibility to design spaces that not only assists healthcare providers but
comforts the patients and families in need of care. He believes the work he does is highly rewarding
when he can create an environment that makes patients and caregivers feel safe, calm, and hopeful.
He also enjoys working with all his clients because their knowledge and passion is infectious, which
motivates him to always go the extra mile.
Changing Demographics in Healthcare: What It Means for Providers
By Brent Johnston, MBA, President of Shared Imaging Services
The United States is entering a transformative era in healthcare, driven by one of the most significant demographic shifts in modern history. By 2030, every member of the baby boomer generation will be over the age of 65—ushering in a historic high for the elderly population. According to the U.S. Census Bureau, one in five Americans will be of retirement age by the end of the decade.
This aging trend has profound implications for healthcare systems, costs, and workforce needs across the nation. The fastest-growing segment of this population—the “oldest old,” aged 80 and above—is projected to increase by nearly 28% between 2025 and 2030. As people live longer, often with multiple chronic conditions, demand for medical services and support will only intensify.
The Wisconsin Perspective
Wisconsin mirrors these national trends, with its own population of seniors expanding rapidly. By 2030, the number of residents aged 65 and older is expected to rise by 30% compared to 2023 levels. The 75+ age group will grow even faster—by an estimated 41%.
This shift means that within just a few years, older adults will represent a far larger share of the state’s healthcare users. For providers, this presents both challenges and opportunities: a greater need for accessible, high-quality care, but also an increasing strain on systems already stretched thin.
The Cost of Care for an Aging America
As the population ages, healthcare costs rise dramatically. The Kaiser Family Foundation reports that Medicare spending for beneficiaries aged 85 and older is nearly twice that of those aged 65 to 74. Data from 2020 further shows that per-person healthcare spending for adults over 85 was 8.5 times higher than for children.
The Centers for Medicare & Medicaid Services (CMS) projects that Medicare spending will grow by an average of 9.7% per year until 2030—driven largely by the baby boomer generation entering retirement. These increases place pressure not only on federal and state budgets, but also on hospitals, clinics, and insurance systems tasked with delivering care efficiently.
Workforce Challenges Ahead
Rising demand for healthcare services comes at a time when the healthcare workforce is shrinking. The Association of American Medical Colleges (AAMC) reports that as many as 40–50% of practicing physicians could reach retirement age within the next decade. Nursing shortages are also a growing concern, with national projections indicating deficits through at least 2037.
By 2027, the United States is expected to face a 10% shortage of registered nurses (RNs)—a gap of more than 200,000 full-time equivalents. The shortages will be most severe in rural, nonmetropolitan areas, where demand for care is often highest and recruitment most difficult.
These shortages ripple across every corner of the healthcare system, from primary care to specialty services like imaging, laboratory diagnostics, and rehabilitation. Providers must increasingly find creative ways to meet patient needs while managing workforce burnout, retirements, and recruitment challenges.
The Growing Role of Imaging Services
Diagnostic imaging plays a central role in managing the health of an aging population. By 2030, nearly 70 million Americans will be 65 or older, and this group already accounts for about 30% of all imaging procedures performed annually.
The most frequently used imaging exams among older adults—X-rays, CT scans, and ultrasounds—are essential for diagnosing and managing conditions such as arthritis, cardiovascular disease, osteoporosis, and cognitive decline. Falls and trauma, common among seniors, also drive significant imaging utilization, as do preventive screenings like coronary calcium scoring and low-dose CT for lung cancer.
As the need for imaging grows, so too does the pressure on hospitals and clinics to deliver timely, accurate diagnostics. The Wisconsin Hospital Association notes that the number of radiologists and technologists entering the workforce is not keeping pace with rising demand. The American Society of Radiologic Technologists (ASRT) reports that the imaging workforce shortage is now the most severe it has been in more than 20 years.
The result is longer wait times for patients, delayed results, and increased workloads for existing staff. Industry forecasters, such as Vizient’s Sg2, predict double-digit growth in imaging utilization over the next decade, including a 14% increase in advanced imaging nationwide.
Bridging the Gap: Shared Imaging Services
For more than 44 years, Shared Imaging Services has been committed to ensuring that rural hospitals and healthcare systems have access to high-quality diagnostic imaging. Founded to bring university-level diagnostics to underserved communities, the organization provides both equipment and staffing for services including nuclear medicine, ultrasound, echocardiography, and MRI.
Through joint ventures and hospital partnerships, Shared Imaging Services helps facilities expand their capabilities without the high costs of ownership. The company’s mobile and on-site solutions not only enhance patient access but also allow hospitals to maintain critical diagnostic services locally—reducing travel burdens and improving care continuity.
In an era defined by demographic change and workforce challenges, collaborations like these will be essential to sustaining quality care. As the population continues to age, the need for innovative partnerships between providers, systems, and diagnostic specialists will only grow.
To learn more about Shared Imaging Services and its work supporting rural healthcare, visit SIS-WI.com.
Creating Ambulatory Surgery Centers That Succeed for Patients, Physicians and Investors

Photo: Modular designs that are easily expandable keep building size and costs low for initial market investments but allow rapid expansion as volumes and market share increase.
By Paul Widlarz and Andrew Zimmer
In the bustling world of modern healthcare, Ambulatory Surgery Centers (ASCs) are carving out a significant niche, offering a more cost-effective and patient-focused alternative to traditional hospital surgical care. But beneath their promise lies a labyrinth of challenges: balancing the diverging needs of stakeholders, navigating regulatory hurdles and planning for uncertain market conditions.
Crafting successful ASCs requires more than just architectural skill; it demands a deep understanding of healthcare dynamics and a collaborative approach to design.
Balancing Stakeholder Priorities
 Take, for instance, the challenge of diverging stakeholder needs. Physicians, as primary users, often emphasize efficiency, valuing workflows that allow them to treat as many patients as possible in a streamlined manner. On the other hand, patients prioritize comfort, privacy and dignity. Investors focus on the bottom line, seeking a balance between upfront costs and long-term returns.
Take, for instance, the challenge of diverging stakeholder needs. Physicians, as primary users, often emphasize efficiency, valuing workflows that allow them to treat as many patients as possible in a streamlined manner. On the other hand, patients prioritize comfort, privacy and dignity. Investors focus on the bottom line, seeking a balance between upfront costs and long-term returns.
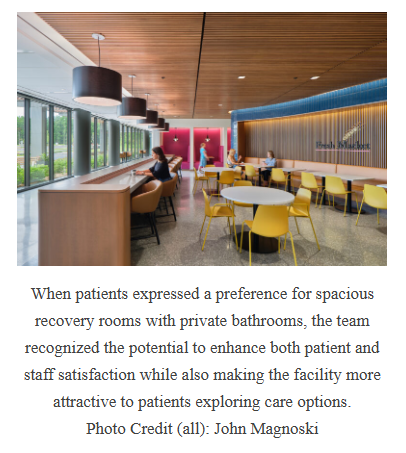
One project for a community health system exemplified this challenge when patients expressed a preference for spacious recovery rooms with private bathrooms—contrasting with the initial design, which prioritized square footage efficiency by omitting dedicated toilet rooms in prep/recovery areas. During later design phases, the team integrated private bathrooms, recognizing their potential to enhance both patient and staff satisfaction while also making the facility more attractive to patients exploring care options.
This balance powerfully reinforced decisions to incorporate natural lighting and comfortable recovery areas to prioritize patient comfort while maintaining efficient staff workflows. The dual focus reduced turnaround times and enhanced patient satisfaction, underscoring the importance of stakeholder alignment at every phase of the design process.
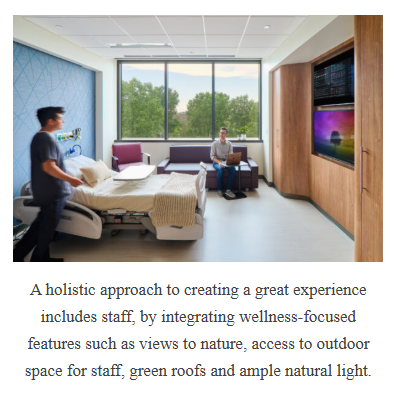
Moreover, a holistic approach to creating a great experience includes staff, by integrating wellness-focused features such as views to nature, access to outdoor space for staff, green roofs and ample natural light.
Operational Strategies to Bridge Gaps
Building on stakeholder alignment, operational strategies often serve as the bridge between diverging goals. For instance, a project focused on physician efficiency adopted a standard, universal operating room (OR) design for all case types, supported by the ability to implement a “waterfall” model, allowing surgeons to alternate between two operating rooms without delay.
In the traditional operational model, physicians alternate between two ORs to maintain their desired throughput, creating tension between provider satisfaction and owner priorities. This approach reduces the number of cases the facility can handle daily and increases space requirements. Waterfall scheduling resolves this conflict by allowing providers to rotate between any available ORs, as all rooms are universal and care teams are cross trained for any case type.
This operational emphasis was also central to nursing team workflows. By implementing streamlined pathways between surgical areas and recovery rooms, the design dramatically reduced non-value-added time for staff, while hospitality-inspired interiors created a welcoming atmosphere for patients. These complementary strategies highlighted how practical and patient-centered approaches can coexist to transform an ASC into a destination center for care.
Navigating Ownership Structures
 With operational strategies in place, ownership structures further shape design considerations. Single-owner systems, such as hospital-led ASCs, often emphasize branding and quality (which can inflate costs), while joint ventures introduce competing priorities between clinical goals and financial imperatives. Modular designs that are easily expandable keep building size and costs low for initial market investments but allow rapid expansion as volumes and market share increase. For example, a new market facility’s initial four operating rooms could adapt to different configurations, supporting immediate operational needs and future growth. This flexibility was particularly valuable for ownership groups focused on scaling operations quickly. Projects that prioritized adaptive layouts allowed for rapid reconfigurations, helping facilities remain competitive in dynamic markets.
With operational strategies in place, ownership structures further shape design considerations. Single-owner systems, such as hospital-led ASCs, often emphasize branding and quality (which can inflate costs), while joint ventures introduce competing priorities between clinical goals and financial imperatives. Modular designs that are easily expandable keep building size and costs low for initial market investments but allow rapid expansion as volumes and market share increase. For example, a new market facility’s initial four operating rooms could adapt to different configurations, supporting immediate operational needs and future growth. This flexibility was particularly valuable for ownership groups focused on scaling operations quickly. Projects that prioritized adaptive layouts allowed for rapid reconfigurations, helping facilities remain competitive in dynamic markets.
Planning for Growth: Overbuilding vs. Underbuilding
As ownership dynamics inform initial designs, planning for future growth ensures that facilities remain viable over time. Flexibility is key when balancing overbuilding and underbuilding. In high-growth markets, ASCs often incorporate shell spaces—unfinished areas reserved for expansion—to adapt to increasing demand. For example, one physician-owned ASC used data analytics to project future growth, aligning facility design with anticipated recruitment goals and surgeon case types. Shell space for future ORs is used today for supplementary support spaces until more surgical capacity is needed.
Overcoming Regulatory Constraints
Beyond growth planning, regulatory constraints add another layer of complexity. Particularly in Certificate of Need (CON) states, ASCs must navigate strict limitations on facility size and scope. Early engagement with regulatory authorities helps ensure compliance without sacrificing design flexibility.
One health system’s approach to adjacent HOPD and ASC platforms demonstrates how strategic site planning and regulatory navigation can enable expansion while maintaining compliance. By aligning outpatient services with hospital-based departments, the outpatient ORs can be billed as HOPD environments today, but easily (and with little cost) converted to ASC billing rates when advantageous or required by payors. Another health system–which built an ASC as a joint venture with a developer and multiple physician groups–thoughtfully segregated provider-based and non-provider-based ORs so that each platform could operate independently adjacent to shared support spaces. These projects demonstrated how thoughtful design can address constraints while fostering innovation.
Lessons in Design Philosophy
From aligning stakeholder priorities to incorporating data-driven decision-making and future-proof modular designs, successful ASCs balance operational efficiency with patient experience. Project teams must remain focused on creating adaptable, efficient spaces that support evolving healthcare demands while fostering environments that promote healing and trust.
Designing ASCs is both an art and a science, requiring teams to navigate a web of competing priorities while delivering spaces that advance healthcare strategies. By weaving together diverse motivations—from patient satisfaction to physician efficiency and investor goals—project teams can create facilities that meet today’s demands and anticipate tomorrow’s needs.
Key Insight for ASC Success
- Stakeholder Alignment: Engage all stakeholders early to reconcile diverging priorities and establish a unified vision.
- Operational Efficiency: Explore strategies like standardized room designs and flexible workflows to enhance productivity.
- Adaptability: Use modular and shell space planning to future-proof facilities for growth and market changes.
- Regulatory Navigation: Collaborate with authorities to ensure compliance while maintaining design flexibility over time.
- Patient-Centered Design: Prioritize comfort and privacy to enhance the patient experience and attract higher-payer demographics.
Paul Widlarz, AIA, principal at HGA, combines a background in medical planning and project management to direct programming, planning, and design processes. Attuned to current research on Lean clinical operations, he works closely with clients and user groups to develop design solutions that optimize healthcare delivery.
Andrew Zimmer, LEED AP, principal at HGA, has extensive experience leading Lean planning engagements at all scales, regionally and nationally. He has spoken about Lean process and planning at the Catalysis Lean Healthcare Transformation Summit in the US and at the Lean Led Hospital Design Seminar for the Lean Association of Finland.
Building a Successful In-house Specialty Pharmacy
By Eric Huckins, Vice President of Business Development, Lumicera
Anyone who has built–or has thought about building–a Specialty Pharmacy for their health system knows it’s not easy. It’s like running a business within a business—you need to have the sophistication required across the entire operation while still being able to deliver on the mission of providing personalized care. There are people to hire, technology systems to learn, contracts to negotiate and don’t forget, accreditation! Whether you’re building from the ground up or want to grow your of your specialty pharmacy faster, there are a few things to consider as you look to bring more revenue into your health system.
Build, Upgrade or Modular? There are options.
This is where the conversations–and the questions–start. If you don’t have an in-house specialty pharmacy, starting one from the ground up can be overwhelming. What if you have a program but aren’t getting the most out of it? Perhaps you have a decent model and just need one area enhanced–how do you find the best options to optimize a particular segment of the business?
Determining whether you have the time, talent and expertise within your system is key to understanding whether you need to bring in a partner to help you achieve your organizational goals.
As you’re making this assessment, here are some of the key departments and areas of expertise you need to consider when determining the best fit your specialty pharmacy program:
Operations
Ensuring this division is well run is vital to your onsite pharmacy’s success. The complexity of managing the prescription workflow requires expertise in data entry, prior authorization, financial support and reimbursement management to achieve optimal turnaround time that patients and providers demand. The dynamics of workload from day-to-day require intricate knowledge and experience to utilize human resources optimally while being precise with the high-dollar inventory management.
Staffing
Whether it’s your front-line staff or the people who ensure everything is working in the background, your specialty pharmacy team is instrumental to your success. Recruiting, training and retaining the right associates are a key part of the specialty pharmacy process. Specialty pharmacies require specialized staff to help with complex processes managing rare diseases, high-cost medications and insurance prior authorizations. Investment in the experience of your staff and the environments where they work pays dividends. And maintaining consistency is important–turnover or labor shortages could affect your patient experience.
Compliance and Risk Management
Knowing and adhering to regulatory standards and mitigating risk are also vital to maintaining a successful specialty pharmacy. As regulatory standards may vary by state, it is important to keep up to date on what is being implemented in the states in which you are dispensing. Additionally, it is critical to implement strategies to minimize medication errors and ensure safe medication practices.
Technology Integration
Technology plays a large part in a successful health system specialty pharmacy model. The journey from receiving the prescription to medication delivery (and all the patient conversations in between) and being able to manage inventory in real time will add to your bottom line. Ensuring you have the right platform to manage the prescription adjudication and deliver your patient management program can make an immense difference in operational efficiency. Your prescribers will be more likely to send their patients to your in-house pharmacy if they’re able to track their prescription and trust your team to deliver for their patients, while ultimately keeping that revenue within your health system.
Clinical Services Enhancement
With specialty pharmacy, service goes beyond dispensing a prescription. Because the disease states are so complex, being able to take the time necessary with a patient to walk them through all the information about their new medication and then developing a personalized journey based on their needs is essential to more positive outcomes. When a patient is happy with the service they’re receiving, they are more likely to return to your specialty pharmacy.
Inventory and Cost Management
Finding ways to trim costs, while still maintaining high levels of efficiency and care can be tricky. Working with your suppliers to secure better pricing and terms for your specialty pharmacy may often rely on higher volumes to realize those savings. If your output is lower, you will need to determine whether you can negotiate the rates you need with manufacturers to realize better savings. Logistics of delivering high-cost, temperature sensitive medication can be a science all its own. Having the right courier contracted at the right rate can drive significant savings and reduce medication replacement risk.
Performance Metrics and Reporting
Your healthcare leaders want to know what’s working and what’s not. That’s why having an analytics reporting platform that can provide on demand metrics and reporting will help keep your specialty pharmacy on track and your leaders in the know. Most specialty pharmacies focus on a variety of key performance indicators such as turnaround times, patient satisfaction and outcomes and budget adherence. Data is imperative for specialty pharmacies to find opportunities for network integrity and to gain access to limited distribution drugs. Finding a partner that has established connections with manufacturers is critical to expanding the patients that can be cared for at the in-house specialty, as well as increase the pull-through of specialty prescription dispenses from patient seen within the system.
Accreditation
Once the pharmacy is up and running, the next milestone is accreditation. When completed, the seals indicate your specialty pharmacy has been held to, and passed, very high standards. It’s one more indicator of the value that’s been put into the process and the care your patients will receive. But the work doesn’t stop at initial accreditation. Ensuring your pharmacy maintains those standards on the path to reaccreditation requires frequent quality monitoring and a routine auditing regimen. Having the formula to gain, maintain and add accreditations is essential for your specialty pharmacy’s success.
Designing a specialty pharmacy, whether it’s a complete build out or just a small segment, is a multi-level, complex process. Lumicera is continually monitoring and implementing best practices to help elevate the specialty pharmacy experience. Our Health Services Solutions team is prepared to offer insights and work alongside those looking to advance their specialty pharmacies. To learn more about our work and the steps we are taking to enhance others’ specialty pharmacies, click here: Health Systems – Lumicera Health Systems or call Eric Huckins, Vice President of Business Development at (608) 716-2667.
It’s Not New Challenges for Healthcare Facilities, Just New Prompts
Author:
Tim Prince, MHA, FACHE
Senior Advisor, Findorff Strategic Insights
Healthcare has never been a static industry. Quality and operational imperatives, evolving payment mechanisms, and unpredictable economics have always challenged administrators to do more with less. That there is challenge in 2025 isn’t really a surprise, but the nature of current prompts come from a new array of factors: materials’ tariffs, market volatility, lead time unpredictability, aging infrastructure, and the pressures of innovation. These demand more strategic, agile facility planning and investment than ever before.
For administrators, the facility is no longer just a backdrop to care: It’s a dynamic tool that can either be a competitive advantage or a liability. And with reimbursement pressures rising and capital increasingly scarce, every square foot must serve a purpose. The role of construction management in this equation is not just technical, it’s strategic.
Volatility in the construction market — from tariffs on materials like steel and copper to disrupted supply chains — has extended lead times and driven costs unexpectedly upward. This volatility can derail even the best-laid capital plans if not addressed proactively. Findorff’s construction experts (ranging from project managers to skilled workers in the field) have deep healthcare expertise that can help mitigate this risk by engaging early, structuring contracts with cost containment mechanisms, and leveraging preconstruction planning to keep projects on time and budget.
At the same time, many hospitals are wrestling with aging infrastructure that hampers clinical efficiency and inflates operating costs. The impulse to delay capital spending is understandable but often shortsighted. Reactive maintenance is expensive, both financially and operationally, and delays with the current market factors only make investments more expensive. Smart investment in facility renewal, guided by life-cycle cost analysis and long-range planning, can pay for itself in resilience, efficiency, and adaptability.
This is where process-innovation and new technologies come into play. Modern construction approaches and techniques allow for faster project execution, fewer change orders, and smoother integration into existing operations. Meanwhile, artificial intelligence and data analytics are beginning to influence everything from early design to post-occupancy performance monitoring, helping administrators make data-informed choices about space utilization, patient flow, and energy use.
For healthcare leaders, the message is clear: Facility investments must be proactive, not reactive; strategic, not transactional. That starts by bringing construction expertise to the table earlier — not just at the design or build phase, but during strategic planning. Doing so allows for alignment between clinical priorities, operational goals, and physical environments.
In today’s climate, healthcare leaders aren’t just being asked to deliver care — they’re being asked to build the future of care. The prompts may be new, but the opportunity remains timeless: to invest wisely, build intentionally, and ensure that the facilities you oversee serve not just today’s patients, but tomorrow’s communities. Let our experts help you find wise, value-driven, impactful ways to assure the right spaces support your excellent care givers.
The Overlooked Part of Healthcare Design: Supporting Staff Through Acoustics (EUA)
Emily Dunn, WELL AP, Prosci | Director of Workplace Strategy, EUA

When we think about designing healthcare environments, we tend to center the conversation around patients and visitors. That’s important—but it’s not the full picture.
Healthcare facilities are workplaces. They’re dynamic, high-pressure environments where caregivers spend long hours navigating urgent situations. Nurses, physicians, and support staff are the backbone of the system. And yet, their well-being is sometimes an afterthought in healthcare facility design.
While hospitals are often the most visible example, these issues apply across a range of healthcare delivery environments—from inpatient wings and emergency departments to outpatient clinics and specialty care centers. In each of these spaces, care providers face intense demands that make designing for staff wellness more than a nice-to-have—it’s essential.
At EUA, we’re seeing more organizations recognize that investment in the experience of their staff and the environments where they work pays dividends in performance, satisfaction and retention. One of the most underperforming, yet impactful, elements of that environment? Acoustics.
Why Sound Matters in Healthcare Workplaces
Many healthcare settings, especially inpatient and high-acuity environments, are inherently noisy places. Alarms, intercoms, rolling carts, overhead pages, conversations in corridors. It adds up to a constant stream of sensory input. Much of that sound has a clear purpose: alerts, notifications, and communication tied to patient care. But when those sounds become overwhelming or unmanaged, they become noise—unwanted sound that can increase stress and decrease performance.
We often talk about how these acoustical environments affect patients. However, the same stressors apply to staff often more acutely, as they experience them hour after hour, shift after shift.
Studies have linked excessive workplace noise to increased stress, fatigue, cognitive overload and even medical errors. In healthcare, where the stakes are high, those impacts carry real consequences, not just for staff well-being, but for patient safety.
The Need for Quiet
What’s often missing from healthcare environments is simple: quiet.
Quiet isn’t just the absence of sound—it’s the ability to step away from the chaos. It enables focus during critical tasks. It may support acoustical privacy, particularly in spaces where sensitive information is shared. And, when it comes to those working in noisy environments, quiet creates opportunities for meaningful respite.
In typical office settings, we’ve grown accustomed to carving out quiet zones, enclosed meeting rooms, or focus pods, even shared library spaces. In many healthcare facilities, particularly inpatient environments, those options are far more limited. Space constraints, tight budgets, and fast timelines often mean staff respite areas are the first to be cut from the program.
But that decision comes at a cost. When staff have no place to recharge—especially during long or overnight shifts—the physical and emotional toll builds quickly. Healthcare providers who experience stress related to their workplace demonstrate lower levels of job satisfaction and higher turnover intention.
Designing with Acoustics in Mind
The good news is that supporting staff and their acoustical needs doesn’t always require a major overhaul. There are small, strategic interventions that can make a big difference:
- Make quiet spaces a priority, not a luxury. Dedicate enclosed, acoustically isolated wellness rooms near staff work zones. These can be compact but effective. Bonus points if they include access to daylight or exterior views, as these help with stress reduction as well.
- Design for visual connection, not acoustical intrusion. In high-acuity areas, consider glazed partitions or windows into adjacent spaces. Seeing the source of a sound can reduce the stress response, even if the sound is still present.
- Balance visibility and privacy. Transparency in design shouldn’t come at the expense of sound control. Use finishes and layout strategies that dampen noise while maintaining situational awareness.
- Account for HIPAA requirements. Acoustic privacy is also a compliance issue. Design spaces where staff can communicate about patient care without the risk of being overheard by outside parties.
As the acoustical experience and the well-being of occupants are important in all environments, we work to regularly integrate these considerations into both workplace and healthcare projects.
Building a Better Culture Through Acoustics
Supporting healthcare staff isn’t just about wellness rooms or sound-absorbing finishes. It’s about signaling that we value their experience and well-being and want to invest in their success.
A focus on the caregiver in a space and working to create a more supportive experience for them in the design process builds culture and community within the workplace. It helps attract and retain top talent in a highly competitive hiring environment. And it contributes to stronger, more sustainable care delivery systems.
We’ve seen this approach work across markets and environments where people regularly operate under pressure and need space to recalibrate.
For instance, many call centers now include wellness rooms for employees who manage emotionally charged conversations. When someone supports callers through personal loss, financial distress, or crises, it’s not sustainable—or healthy—to jump from one call to the next without pause. Giving employees the option (and a space) to step away for a few minutes allows them to process, recover, and return to their work with a clearer head and renewed empathy. That sense of empathy is essential to doing the job well, and it’s precisely the kind of quality we should be protecting through thoughtful workplace design.
We also see this in academic medical centers and other high-acuity care environments, where students and residents often have access to small, quiet spaces near clinical areas. These rooms offer a moment of privacy after a difficult encounter or a misstep in care—opportunities to regroup, reflect, and regain composure before re-entering a high-stakes environment. These moments are critical not only for mental health but for learning. By normalizing the need for pause, we build emotional resilience and reinforce a culture of support and accountability.
These examples highlight what’s possible when we intentionally design for staff experience. They remind us that high performance and well-being aren’t at odds—they’re interdependent.
Let’s Keep the Conversation Going
We know healthcare environments will always be complex. But that doesn’t mean they can’t be restorative for everyone inside them.
Let’s design workplaces where caregivers can thrive. Let’s put acoustics higher on the priority list.
Emily Dunn, WELL AP, Prosci, is the director of workplace strategy at EUA. She is a member of the WELL Sound Concept Advisory.
Designing a Positive Pediatric Experience for Patients and Families
The patient and family experience encompasses various interactions and environments, from provider interactions influenced by institutional policies to the impact of the physical surroundings on emotional and physiological well-being. Designing pediatric care spaces requires recognizing children’s unique needs and integrating families into their care journey. Creating positive experiences involves considering key spaces and elements throughout the facility.
Arrival Welcome:
The first impression begins before entering a facility. When children arrive with their family, emotions and stress run high for all. To help reduce patient and family stress on arrival, clear navigation, distinctive facility identity, and stress-reducing measures should be considered like intuitive parking, entryways, and wayfinding to inspire confidence and create the shortest paths.

Public Spaces:
Make the experience an adventure. Design should cater to children’s perspectives and needs, creating a comfortable and welcoming environment. Inviting seating cubbies, locally inspired art, graphically compelling wayfinding, and low-tech and high-tech interactive features such as video walls can engage children as they move through waiting and common spaces.
Patient Encounters:
Tailored spaces, from patient rooms to procedure areas, greatly affect a child’s well-being. Patient rooms should offer elements of control and comfort akin to home, while procedure rooms benefit from designs that mitigate stress through soothing aesthetics and distraction.


Family Spaces:
Parents, siblings, and extended family members all move through the system alongside the patient. Inclusive designs accommodate diverse family needs offering contemplative areas, places for an adult private moment, work or call, varied seating that accommodates adults and children, access to daylight and the outdoors including sibling play areas, and family amenities like private showers and kitchenettes. Considerations extend to religious practices and dietary needs, reflected in facility features such as kosher kitchens and interfaith centers that support healing and care.
Indoor/Outdoor Connection:
Biophilic design elements bridge indoor and outdoor spaces, enhancing comfort and providing opportunities for therapeutic programs. Safety considerations prioritize staff visibility and protection from the elements, while outdoor zones can support activities like physical therapy and community engagement.

Lasting Impression:
Departure experiences should be intuitive and welcoming, leaving a positive lasting impression. Clear check-out processes and friendly staff interactions contribute to a seamless transition from hospital to home.
Designing a pediatric facility that best meets the needs of the children, their families, and staff, is a complex process. HGA continues to examine trends shaping pediatric care, develop planning and design strategies that elevate environments, research the impact of these design interventions, and share our learnings. Learn more about our work and the steps we are taking to create environments that foster healthy outcomes and overall wellbeing for patients, families, and staff.
(Based on article on Insights: https://hga.com/designing-a-positive-pediatric-experience-for-patients-and-families/)

